“What’s the craziest thing you’ve experienced in the ER?”
I’m often asked that question when people find out I practice emergency medicine. I became a doctor because I find great fulfillment in the charge and challenge of helping people who are suffering. Though I’m sure innocent curiosity drives that inquisitiveness, sharing the suffering of others not only violates the delicate trust people share with me but also reopens painful memories I’ve learned to compartmentalize in order to cope with daily heartache.
I care for people in their most vulnerable states, on their worst days, sometimes in their last hours.
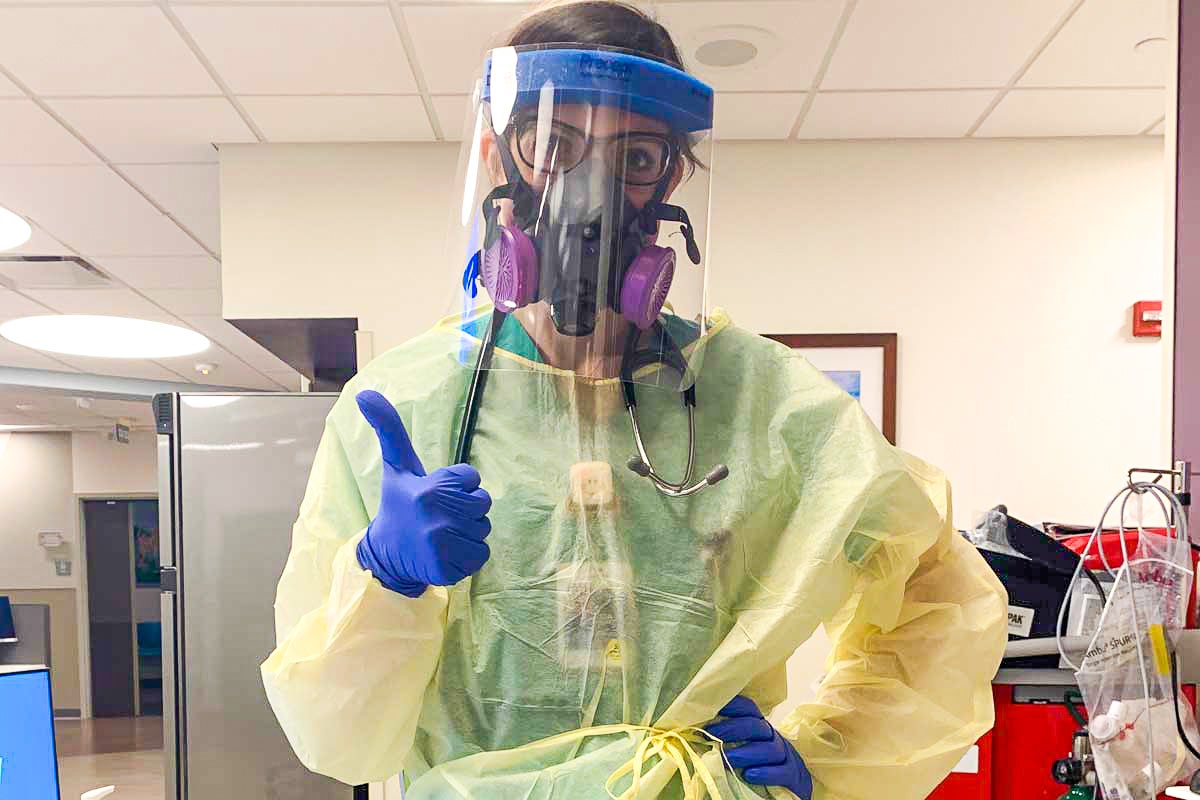
I’m not naïve to hazards and uncertainties. This isn’t the first time I’ve gowned and gloved and masked. I’ve worn plenty of PPE caring for patients with tuberculosis, meningitis, blood borne pathogens and infectious disease.
During the 2013-2014 H1N1 influenza outbreak, I was a tender intern and first experienced the sobering reality of caring for young, healthy patients my age, dying in the ICU on ventilators and maximal critical care support.
“This is the craziest thing I’ve ever experienced in the ER. ”
I’m not a stranger to bad news and difficult situations. This isn’t the first time I’ve seen fear in the eyes of my patients.
“The CT scan showed what we were dreading… You have cancer.”
“I’m doing everything I can to help your mom get better, but nothing is working and she keeps getting sicker.”
“We need to talk about what to do if your breathing becomes worse. The next step would be to put you on a ventilator — life support.”
“I’m so very sorry to have to tell you that your husband has died.”
“I can’t find your baby’s heartbeat. It breaks my heart to say that you’re having a miscarriage.”
This is, however, the first time that I have felt inadequate in using my knowledge and skills to assess risk and anticipate what is to come. No one alive can provide first-hand experience or advice.
This virus is so puzzling because it spreads so quickly, it knows no boundaries, it stealthily infects and presents with a broad spectrum of symptoms. No population is safe.
This is the craziest thing I’ve ever experienced in the ER.

Prior to the arrival of COVID-19 at my hospital, my husband and I discussed a game plan to prepare for a worst-case scenario. I’m following guidelines and using equipment to prevent exposure to my husband and our 11-month-old baby, but in reality, not much has changed in my everyday actions to prevent the spread of illness that I encounter at the hospital during a normal ER shift.
I have been and will continue to do my best to keep us all healthy and safe. We are currently self-isolating to protect our family, our friends and our community.
I’m not scared. I have faith in God and the graces that will arise from this situation if we allow it. I’m controlling what I can, and I’m not worrying about what I cannot.
Our ER patient volume is currently down at my facility. I’m hoping that it’s because people are paying heed and isolating.
All masks at my hospital are now under lock and key. I am rationed one surgical mask per shift to wear. N95s are a commodity. I was fitted for a non-disposable p100 mask a couple of weeks ago, but the filter cartridges have a 40-hour life. We have no replacements for them as of now. I tried to buy some on my own, but they’re all sold out online.
“The anxiety at work is palpable. We’re quietly waiting for the tsunami to hit.”
The anxiety at work is palpable. We’re quietly waiting for the tsunami to hit.
Projections we are using to prepare predict that our wave won’t crest here until early to mid-April, and the onslaught of the sickest patients will continue into May. We already have crisis tents set up in the hospital parking lot, awaiting the surge.
“Social distancing” feels ridiculous. It should. If it’s difficult, it means that you’re doing it right. A virus needs a host to survive, to replicate, to spread. If everyone would self-isolate, this pandemic would end rapidly. Coronavirus would have nowhere to move to continue its wrath.
So I’m begging you — please stay home.
Stay home for grandmas, for transplant patients, for doctors and nurses, for respiratory therapists and first responders. For cleaning crews and grocery store employees and gas station attendants, for Instacart and Amazon workers. For small business owners and the currently unemployed.
Stay home for me. For my husband and baby. Please help to protect us.
You have the opportunity — and the responsibility now — to help save lives, too.
Jessica Goldonowicz DeSalvo ’09 is a board certified emergency medicine physician currently practicing in Central Florida. She earned her bachelor’s degree in molecular biology and microbiology as a Burnett Honors Scholar in 2009. Jessica is wife to Eric DeSalvo ’09, UCF assistant athletics director of #Content, and mama to Sebastian.